Bone Grafting vs Dental Implants: Which Is Better for Successful Dental Implant Procedures?
Bone grafting and dental implants are complementary components of oral rehabilitation: bone grafting restores or augments jaw bone volume, while dental implants replace missing tooth roots to support crowns or prostheses. This article explains how bone grafting and implants work, when grafting is necessary, and how each approach affects recovery, success rates, and long-term function for patients considering implant-based tooth replacement. Many adults face jawbone loss after extractions, periodontal disease, or trauma, and understanding osseointegration and bone volume requirements is central to choosing the right path. We will walk through procedural steps, compare graft materials, outline recovery timelines, present cost considerations, and summarize clinical decision factors so you can weigh grafting plus implants versus implant-only strategies. Throughout, related concepts such as sinus lifts, ridge augmentation, CBCT imaging, and minimally invasive alternatives are explained in patient-friendly terms, and practical checklists and tables help clarify trade-offs. After an educational review of options, readers who want a personalized assessment can learn how a local Grand Prairie dental office evaluates bone needs and plans implant treatment with a free consult.
What Is the Role of Bone Grafting in Dental Implant Procedures?
Bone grafting restores structural support to deficient jaws so implants can achieve primary stability and long-term osseointegration. In clinical terms, bone grafting addresses inadequate bone height, width, or contour by adding graft material that acts as a scaffold for new bone formation; this process improves implant anchorage and prosthetic outcomes. Common indications include alveolar ridge resorption after tooth loss, periodontal bone defects, trauma, and areas where sinus pneumatization limits vertical height. Restoring volume also optimizes esthetics in the anterior zone by supporting soft tissue contours and preventing implant exposure. Understanding the role of grafting clarifies why some implant cases are straightforward while others require staged reconstruction before implant placement.
Bone grafting procedures begin with diagnostic imaging and end with a phase of biological integration that precedes or accompanies implant placement, which we will explain next to clarify patient expectations and timeline.
How Does the Dental Implant Bone Graft Procedure Work?
Bone grafting for implants begins with a clinical exam and three-dimensional imaging, typically a CBCT scan, to define bone volume and anatomic limits. The surgical sequence commonly includes local anesthesia, flap design or flapless access, placement of graft material (particulate or block), stabilization with membranes or fixation screws when needed, and tension-free soft-tissue closure to protect the site during healing. The graft material serves as an osteoconductive scaffold and, depending on type, may also provide osteoinductive signals that recruit host cells to form new bone. The healing interval varies by graft type and location, after which the clinician evaluates integration and proceeds with implant placement either in the same surgery (simultaneous) or after a delayed interval to allow maturation. Patients typically experience manageable post-op symptoms and return for follow-up visits to monitor integration, which we will discuss in recovery and timeline sections.
This procedural overview leads naturally to understanding differences among graft sources and materials, which affect handling, healing, and clinical choice.
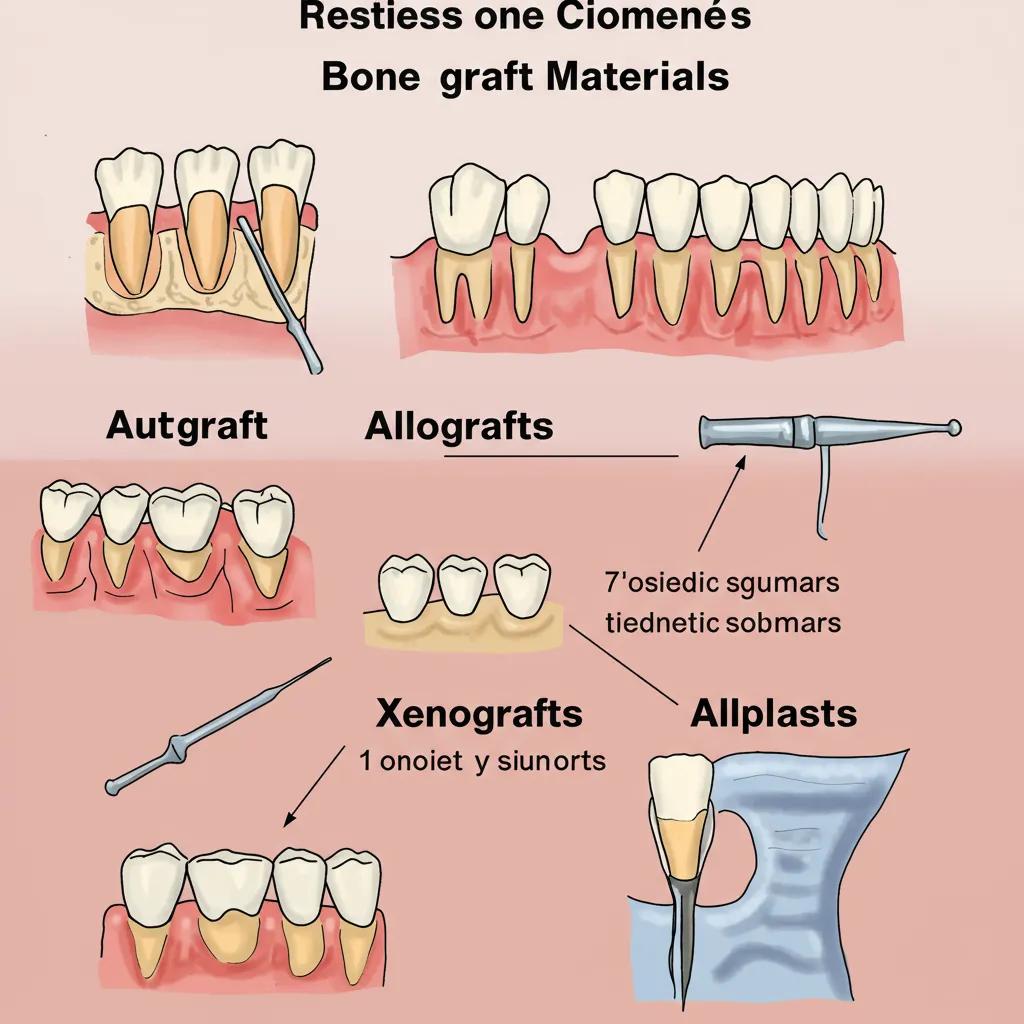
What Are the Types of Bone Grafts Used for Dental Implants?
Clinicians choose among autografts, allografts, xenografts, and alloplastic grafts based on defect size, patient preference, and desired healing characteristics. An autograft uses the patient’s own bone—often from the jaw or hip—and provides living cells and growth factors, making it the gold standard for biological potential but requiring a donor site. An allograft is donor human bone that is processed to be safe and widely available; it reduces operative morbidity but has different remodeling timelines. Xenografts derive from another species and act primarily as a scaffold with slower resorption. Alloplasts are synthetic materials engineered for predictable handling and absence of disease transmission risk. Each option influences healing speed, resorption profile, and likelihood of rapid osseointegration for the subsequent implant.
To compare these materials side-by-side and set realistic expectations, the table below summarizes source, pros, cons, and typical healing time.
Graft Type
Source / Description
Pros
Cons
Typical Healing Time
Autograft
Patient’s own bone (intraoral or extraoral)
Osteogenic + osteoinductive, high integration
Donor-site morbidity, longer surgery
3–6 months (site dependent)
Allograft
Processed human donor bone
Readily available, no donor-site surgery
Variable remodeling speed, less living cells
4–6 months
Xenograft
Animal-derived mineral scaffold
Long-lasting scaffold, good volume maintenance
Slower resorption, may integrate slower
6–9 months
Alloplast
Synthetic ceramics/polymers
No disease transmission, predictable supply
Less biologically active, depends on adjuncts
4–9 months (varies)
This comparison helps patients and clinicians match clinical goals to material choice and leads into how grafting affects recovery and final implant success.
How Does Bone Grafting Affect Dental Implant Recovery and Success Rates?
Bone grafting extends the timeline of implant therapy because graft sites require biologic integration before implants can reliably support prostheses, but grafting also increases candidacy and long-term implant stability. The primary mechanism is structural: additional bone volume enhances primary stability at implant placement and provides better load distribution during osseointegration. Clinically, grafted sites can convert previously unsuitable anatomy into predictable implant sites and reduce complications like implant exposure or failure. Recovery includes immediate soft-tissue healing followed by a longer bone remodeling phase; patient factors such as smoking, systemic health conditions, and oral hygiene materially affect healing and ultimate success rates. Recent clinical perspectives emphasize individualized risk assessment and close follow-up to optimize outcomes.
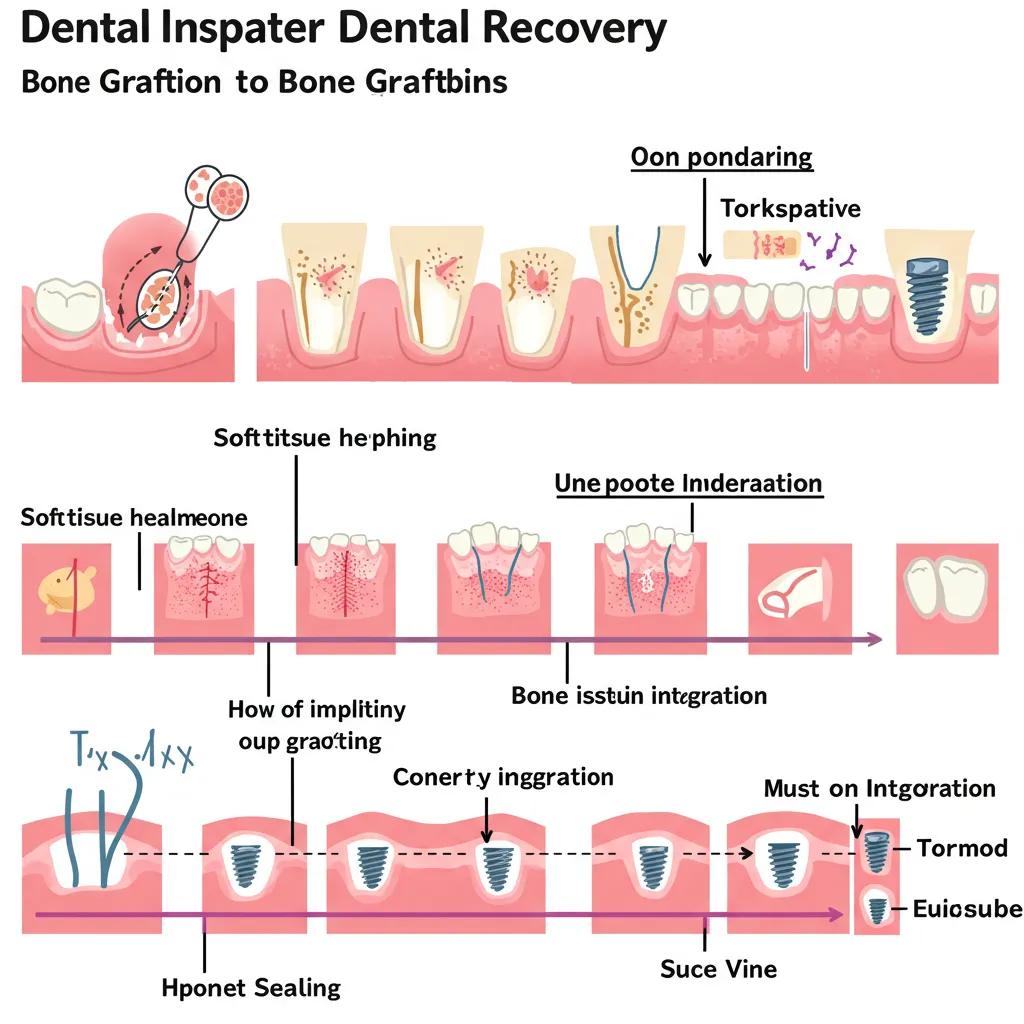
Below is a clear patient-centered timeline summarizing typical stages from immediate post-op care to implant readiness and long-term integration.
0–2 weeks: Acute soft-tissue healing with swelling control, pain management, and diet modifications.
1–3 months: Early graft consolidation; provisional restorations avoided in graft zones to reduce load.
3–6 months: Ongoing graft integration and new bone formation depending on material; implant placement often considered.
6+ months: Mature bone remodeling and definitive prosthetic loading when imaging and clinical tests indicate readiness.
This staged recovery timeline leads into how grafting specifically improves implant success rates through biomechanical and biological effects.
What Is the Bone Graft for Dental Implant Recovery Timeline?
A realistic recovery timeline balances patient expectations with biological processes: soft tissues typically heal within two weeks, while bone graft integration unfolds over months. Initial postoperative care focuses on limiting swelling and protecting the graft—cold packs, soft diet, and prescribed medications help during the first 7–14 days. Bone formation and vascular ingrowth begin in the first month and progress through months two to six, with radiographic signs of consolidation guiding the clinician. Depending on graft type and location—sinus lifts or large block grafts may need up to six to nine months—implant placement timing is individualized. Patients should expect staged check-ins and imaging to confirm readiness before the implant is placed.
Knowing this timeline helps patients plan work and lifestyle adjustments during healing and transitions naturally to how grafting contributes to higher implant stability and long-term success.
How Does Bone Grafting Improve Dental Implant Success Rates?
Bone grafting improves implant outcomes by creating sufficient native bone volume for secure initial implant fixation and by fostering an environment conducive to osseointegration. Primary stability—mechanical engagement at the time of implant insertion—is strongly correlated with early and lasting osseointegration; grafted sites that achieve adequate volume and density allow implants to reach the insertion torque and contact necessary for success. Grafting also reestablishes alveolar contours that support soft tissues, reducing recession and esthetic complications. Success rates are further affected by proper surgical technique, choice of graft material, and patient health; when these factors align, grafting lowers the risk of implant failure and peri-implant complications. Clinicians reduce risk through meticulous sterile technique, appropriate material selection, and staged planning when required.
Can You Get Dental Implants Without a Bone Graft?
Yes — in many cases dental implants can be placed without additional bone grafting when native bone volume and density are sufficient for primary stability and long-term support. The deciding factors include available bone height and width as assessed on CBCT imaging, bone quality, occlusal forces, and the prosthetic plan. Alternative strategies such as short implants, angled implants, or implant-supported overdentures may allow implant therapy without grafting in selected situations, reducing surgical complexity and recovery time. However, candidacy for graft-free options requires individualized assessment; an implant placed in marginal or insufficient bone may risk early failure or esthetic compromise, so clinical judgment and imaging guide the approach.
Below we list common graft-free implant strategies, their practical uses, and limitations to help readers understand alternatives and why a consult matters.
Short implants: Shorter fixtures placed where vertical bone is limited that avoid extensive augmentation in many cases.
Angled implants (tilted implants): Strategic angulation to engage available bone and avoid anatomic obstacles.
Mini implants: Narrow-diameter implants for limited-support scenarios or as transitional solutions.
These graft-free options illustrate that implant strategies can adapt to anatomy, and scheduling an evaluation helps determine which approach fits a given patient’s needs and anatomy.
What Are the Dental Implant Without Bone Graft Options?
When bone volume is limited but adequate in key dimensions, clinicians may use short or specially designed implants and prosthetic strategies to avoid grafting. Short implants reduce the required vertical height, making them suitable for posterior areas with limited bone, while angled implants can engage denser bone in different regions to bypass deficient ridges or sinuses. Mini implants offer less invasive placement for temporary or limited-support uses, although they may not suit high-load permanent restorations. Each graft-free option balances biomechanical trade-offs—short implants can perform well in controlled circumstances, angled implants require precise planning and prosthetic compensation, and minis are often adjunctive. Choice of technique depends on CBCT findings, occlusal demands, and the broader treatment plan.
Understanding these clinical alternatives leads to the clear criteria that define when grafting is truly unnecessary, which we cover next.
When Is a Bone Graft Not Necessary for Dental Implants?
A bone graft is typically unnecessary when CBCT imaging shows adequate bone height, width, and density to achieve primary stability and to support the intended prosthesis without compromising esthetics or function. Specific clinical criteria include sufficient cortical and cancellous bone around the planned implant trajectory, absence of active infection or periodontal pockets in the area, and systemic health conditions that support healing. When prosthetic demands are modest—such as single posterior teeth with favorable bite dynamics—clinicians may choose implant designs that avoid grafting. Patient preferences regarding fewer surgeries and shorter timelines also weigh in, but final determination rests on objective imaging and clinical testing.
Clear diagnostic steps flow from these criteria, emphasizing why a professional assessment is necessary to confirm candidacy for graft-free implant options.
What Are the Costs Involved in Bone Grafting for Dental Implants?
Bone grafting costs vary because procedures differ in complexity, graft material, surgical expertise, and facility use; presenting ranges helps patients budget while reinforcing that personalized estimates require a consult. Major cost drivers include graft type (autograft vs allograft vs xenograft vs alloplast), procedure complexity (sinus lift, ridge augmentation, block graft), surgeon fees, anesthesia and facility costs, and follow-up imaging or temporary prosthetics. Insurance coverage is inconsistent: some plans may cover grafts when deemed medically necessary, while many dental benefits treat grafting and implants as elective or subject to annual limits. For clarity, the following table gives typical ranges and factors that influence price variability and insurance considerations.
Below is a concise cost table to orient readers while reinforcing that exact pricing requires individualized assessment.
Procedure
Typical Cost Range (USD)
Factors That Affect Cost
Insurance Considerations
Minor particulate graft (small socket augmentation)
$300–$1,200
Graft material, site size, surgeon fees
Often out-of-pocket; insurance varies
Sinus lift (lateral window)
$1,500–$3,500
Extent of lift, graft type, anesthesia
Sometimes partially covered if medically necessary
Ridge augmentation / block graft
$1,000–$4,000
Donor site requirement, fixation hardware
Typically limited coverage; preauthorization advised
Autogenous graft with donor site
$2,000–$6,000
Donor site, operative time, hospitalization if extraoral
More likely to be considered medically necessary in some cases
This cost overview shows variability and highlights why a personalized consult is essential to receive an accurate estimate and to discuss financing or insurance questions.
How Much Does the Cost of Bone Graft for Dental Implant Vary?
Price variability stems from the size and complexity of the defect, the choice of graft material, whether a donor site is needed, clinician expertise, and regional fee differences. Small socket grafts are relatively economical, whereas extensive block grafts or sinus lifts require more surgical time, specialized materials, and possibly additional visits, raising costs. The selection of biologics or growth factor adjuncts, use of resorbable membranes, and need for fixation hardware add incremental expenses. Facility and anesthesia fees also vary by practice setting. Because each case presents unique needs, clinicians commonly recommend a free consult to review imaging and provide a tailored cost estimate that accounts for both clinical and financial considerations.
Recognizing this variability clarifies why checking insurance benefits and scheduling a consult are practical next steps for most patients.
Are Bone Grafts Covered by Insurance for Dental Implants?
Insurance coverage for bone grafts is inconsistent: some medical plans may cover grafting when it is part of a medically necessary reconstructive sequence, while many dental plans consider grafts and implants elective and apply limitations or exclusions. Coverage often depends on documentation of medical necessity, coding, and whether associated procedures intersect with medical diagnoses. Patients should review their benefits carefully and obtain preauthorization when possible; clinicians typically provide itemized treatment plans and supporting documentation to assist with claims. A free consult at a dental office can help clarify likely out-of-pocket costs and the potential for insurance involvement based on the individual case.
What Are the Benefits and Risks of Bone Grafting Compared to Dental Implants Alone?
Combining bone grafting with implants offers key benefits—restored bone volume, improved primary stability, and better esthetic outcomes—but it also adds surgical complexity, extended healing time, and potential for graft-specific complications. Benefits include enabling implant placement in previously unsuitable sites, enhancing soft-tissue support for better gingival esthetics, and reducing long-term biomechanical complications by creating a stable foundation. Risks include infection, graft failure or resorption, prolonged healing, and donor-site morbidity for autografts; implant-only approaches avoid those graft-specific risks but may be limited by anatomy or long-term prosthetic compromises. Clinicians manage risks through careful patient selection, aseptic technique, appropriate material choice, and staged planning when indicated.
To illustrate trade-offs clearly, the table below contrasts outcomes, benefits, and likelihood notes for grafted versus non-grafted approaches.
Outcome
Benefit (with graft)
Risk/Downside (with graft)
Likelihood / Notes
Primary implant stability
Higher in augmented sites when volume restored
May require delayed implant placement
Likely if graft integrates
Esthetic contour
Improved soft-tissue support in anterior cases
Additional surgery extends timeline
Important for esthetic zones
Surgical morbidity
Restores anatomy
Donor-site issues possible with autograft
Variable by graft type
Overall treatment time
Longer due to healing intervals
Extended treatment may affect patient schedule
Common in staged reconstructions
This balanced comparison supports a reasoned decision-making process that prioritizes long-term implant prognosis and patient priorities.
What Are the Advantages of Combining Bone Grafting with Dental Implants?
Combining grafting with implants expands treatment possibilities by recreating deficient anatomy and allowing implants to be positioned optimally for function and esthetics. Grafting increases the bone available for implant anchorage, which improves initial mechanical stability and promotes predictable osseointegration. Reconstructing the ridge contour supports soft tissues and prevents future recession, which is especially important in the anterior smile zone for esthetic outcomes. Clinically, grafting can transform a complex restorative problem into a predictable rehabilitative sequence, enabling implant-supported crowns, bridges, or overdentures with durable function. These advantages, when weighed against added procedures and timelines, often favor grafting when long-term prognosis and esthetics are priorities.
These advantages lead naturally to a discussion of potential complications and how they are mitigated.
What Are the Potential Risks and Complications of Bone Grafting?
Common complications include infection, graft exposure, partial resorption, and insufficient integration that may necessitate revision surgery; rarer events include sensory disturbances if nerves are near the donor or recipient site. Early signs of complication often involve increased pain, persistent swelling, wound dehiscence, or drainage, and clinicians address these promptly with antibiotics, debridement, or modification of the treatment timeline. Donor-site morbidity for autografts can cause additional discomfort or morbidity that must be discussed preoperatively. Clinicians reduce complication likelihood through strict sterile technique, careful flap management, appropriate tension-free closure, judicious material selection, and thorough preoperative planning to avoid anatomic hazards. Patient adherence to aftercare—smoking cessation, oral hygiene, and follow-up—also markedly influences outcomes.
With risks and benefits understood, patients need a decision framework to choose the best path for their individual situation, which is the next focus.
How to Decide Between Bone Grafting and Dental Implants: Which Is Better for You?
Choosing between bone grafting plus implants and implant-only strategies depends on patient-specific medical factors, anatomic findings on imaging, prosthetic goals, esthetic priorities, and tolerance for surgical stages and treatment duration. Clinicians typically follow a diagnostic workflow—CBCT imaging, periodontal assessment, occlusal analysis, and medical history—to determine whether augmentation is required to achieve functional and esthetic objectives. Patients should consider systemic health issues (e.g., diabetes control), smoking status, financial implications, and how treatment timelines fit life responsibilities. Shared decision-making between patient and clinician, sometimes involving a specialist referral for complex grafting or advanced implant designs, ensures the selected plan balances risk, benefit, and patient values. A clear checklist helps patients prepare for consults and fosters informed choices.
These decision factors flow into the clinical evaluation process clinicians use to recommend grafting or alternative implant strategies, which we describe next and include an invitation for personalized planning with a local provider.
How Do Dental Professionals Evaluate Candidates for Bone Grafting vs Implants?
Evaluation begins with a comprehensive medical and dental history, followed by clinical exam and three-dimensional imaging—CBCT scans—to quantify bone volume and map anatomic constraints such as the sinus floor or mandibular canal. Periodontal charting checks for active disease, while occlusal analysis identifies bite forces that influence implant selection and prosthetic design. Based on these data, the clinician models implant positions, decides whether grafting or alternative implant designs are needed, and outlines a staged timeline including expected healing intervals. This structured workflow ensures decisions rest on objective imaging, functional demands, and patient priorities rather than on assumptions, enabling clear informed consent and planning for successful outcomes.
After clarifying evaluation steps, readers often ask about innovations that can minimize invasiveness or accelerate healing, which we address next.
What Are the Latest Advances in Bone Grafting and Dental Implant Techniques?
Recent advances focus on biologics, improved graft materials, and minimally invasive surgical techniques that reduce patient morbidity and enhance predictability. Biologics such as platelet-rich fibrin (PRF) or growth factor concentrates augment graft biology by concentrating autologous cells and proteins that promote vascular ingrowth and regeneration. Material science has produced composite grafts and resorbable membranes with improved handling and barrier function, while computer-guided implant planning and surgical guides increase placement accuracy. Minimally invasive instrumentation—piezosurgery and flapless techniques—reduces soft-tissue trauma and accelerates recovery. These innovations collectively improve patient experience and expand the range of cases treatable with less morbidity.
How Are New Materials Improving Bone Graft Procedures?
Contemporary biomaterials optimize resorption profiles, osteoconductivity, and handling characteristics to support predictable bone formation while minimizing the need for repeat procedures. Composite grafts combine synthetic scaffolds with biologic adjuncts to marry mechanical stability with biological activity, and resorbable collagen membranes now better preserve graft shape while preventing soft-tissue ingrowth. Advances in membrane design and fixation reduce micromotion that can compromise integration, and engineered ceramics provide tailored pore architecture that supports vascular infiltration. These material improvements translate to faster integration, more predictable volume maintenance, and easier surgical handling, which collectively benefit patients by reducing complication rates and supporting reliable implant placement.
Material improvements set the stage for less invasive surgical approaches that further enhance recovery, which we describe next.
What Minimally Invasive Options Are Available for Bone Grafting and Implants?
Minimally invasive techniques include guided bone regeneration with smaller flaps, flapless implant placement when anatomy permits, piezoelectric instrumentation to reduce bone trauma, and computer-guided implant surgery to shorten operative time and increase precision. Ridge expansion with specialized osteotomes or split-crest techniques can augment narrow ridges without large block grafts, reducing donor-site morbidity. Guided surgery allows prefabricated provisional restorations and precise implant angulation, which can minimize postoperative discomfort and speed rehabilitation. These approaches, when combined with appropriate biologics and careful planning, decrease soft-tissue trauma and support faster patient recovery while maintaining treatment predictability.
Having explored advances, it is essential for patients to understand how to protect grafts and implants during recovery; the next H2 outlines practical aftercare instructions.
How to Care for Your Dental Implants After Bone Grafting?
Effective aftercare protects graft integrity, supports osseointegration, and reduces complication risk through a combination of immediate postoperative measures, staged oral hygiene, and timely follow-up evaluations. Immediate care emphasizes cold packs to control swelling, a soft diet to avoid load over the grafted area, and adherence to prescribed medications including analgesics and, when indicated, antibiotics. Oral hygiene should be adapted to protect the surgical site—gentle rinses and avoidance of mechanical trauma in the graft zone—while routine plaque control elsewhere continues. Smoking cessation and management of systemic conditions are crucial because these factors directly affect vascularity and healing. Regular follow-up appointments and imaging allow clinicians to confirm graft consolidation and plan subsequent implant placement.
Next we present an actionable aftercare checklist that patients can follow day-by-day and week-by-week to support healing and successful implant outcomes.
What Are the Best Practices for Bone Graft and Implant Aftercare?
Aftercare best practices include strict adherence to medication regimens, protective diet choices, adapted oral hygiene, and activity modifications to minimize complications and support vascularization of the graft. Patients should take prescribed analgesics and any adjunctive antibiotics as directed and use recommended antiseptic rinses once the clinician allows to reduce infection risk. A soft, nutrient-rich diet for the first 1–2 weeks prevents undue pressure on the graft, and avoiding heavy lifting or strenuous exercise reduces the chance of bleeding or wound disruption. Gentle toothbrushing near adjacent teeth and avoidance of the surgical site preserve healing tissues until soft tissue closure is secure. Finally, smoking cessation and glycemic control are essential for predictable bone regeneration and osseointegration.
Following these practices prepares patients to recognize when complications require prompt attention, which the next subsection outlines.
When Should You Contact Your Dentist After Bone Grafting and Implant Surgery?
Patients should contact their dental provider promptly for signs indicating possible complications, including increasing or severe pain unrelieved by medication, fever of 101 degrees Fahrenheit (38.3 degrees Celsius) or higher, spreading or increasing swelling after the first 48–72 hours, persistent bleeding that does not respond to gentle pressure, or purulent drainage from the surgical site. Altered or worsening sensation (numbness or tingling) in the lip, chin, or tongue that does not improve should be reported immediately, as should any suture dehiscence or visible graft exposure. Routine follow-up visits are typically scheduled within the first week, at one month, and periodically during the graft integration phase to monitor progress and intervene early if needed. Timely communication with the treating team ensures complications are managed quickly and reduces the risk of implant compromise.
For patients who want a personalized treatment plan after reading this guidance, the following section outlines how to move from information to action.
Bone grafting and dental implants together restore function and esthetics when planned and executed correctly, and a free consult with a Grand Prairie dental office can clarify whether grafting is needed and which implant strategy best fits your anatomy and goals. The Grand Prairie dental office provides implant planning and denture services and evaluates bone needs with imaging and clinical assessment to recommend grafting, graft-free options, or minimally invasive alternatives. Scheduling a free consult allows a clinician to review your CBCT imaging and develop a personalized timeline and cost estimate. This final step translates the decision framework in this article into a concrete plan tailored to your clinical condition and preferences.
Guided Bone Regeneration for Dental Implants Utilizing Platelet-Rich Fibrin
Guided bone regeneration (GBR) is a well-established and predictable technique for achieving vertical and horizontal bone augmentation to address bone defects prior to implant placement. However, variations in protocols can lead to differing clinical outcomes. Platelet-rich fibrin (PRF) has been proposed as a means to enhance the results of regenerative procedures. Therefore, this study sought to characterize the bone gain achieved with GBR protocols that incorporate membranes, bone grafts, and PRF for both vertical and horizontal bone augmentation.
Guided bone regeneration in staged vertical and horizontal bone augmentation using platelet-rich fibrin associated with bone grafts: a retrospective clinical study, M Freitas Monteiro, 2020
Recent advances focus on biologics, improved graft materials, and minimally invasive surgical techniques that reduce patient morbidity and enhance predictability. Biologics such as platelet-rich fibrin (PRF) or growth factor concentrates augment graft biology by concentrating autologous cells and proteins that promote vascular ingrowth and regeneration. Material science has produced composite grafts and resorbable membranes with improved handling and barrier function, while computer-guided implant planning and surgical guides increase placement accuracy. Minimally invasive instrumentation—piezosurgery and flapless techniques—reduces soft-tissue trauma and accelerates recovery. These innovations collectively improve patient experience and expand the range of cases treatable with less morbidity.
Xenograft Versus Alloplast Bone Grafts for Infrabony Defects
Currently, several surgical therapies are available for treating infrabony defects, including bone grafting. However, numerous factors influence the selection of the optimal bone graft material. This study aimed to compare the effectiveness of xenograft and alloplast bone grafts in the therapy of infrabony defects. The allograft demonstrated a significantly greater amount of newly formed bone compared to the xenograft. No significant differences were observed in the percentage of newly formed bone between the allograft and the alloplastic graft, nor between the alloplastic graft and the xenograft. Among the three graft types, no discernible changes were noted in the percentage of remaining particles. All bone substitute materials exhibited…
Comparison of xenograft and alloplast bone grafts for infrabony bone defect: Literature review, M Amalia, 2023