Dental Implant Vs Crown Longevity: Comprehensive Guide to Lifespan and Cost for Mansfield Patients
Dental implants and dental crowns address tooth loss and structural damage with different biological and mechanical approaches, and understanding how each option performs over time helps patients in Mansfield make informed restorative choices. This guide explains what dental implants and crowns are, how their components and materials influence longevity, and which clinical and lifestyle factors most strongly predict long-term success. Many patients face the trade-off between higher upfront cost and longer functional life when choosing between implant-based tooth replacement and crown-based restoration; this article clarifies those trade-offs with practical timelines, maintenance strategies, and cost comparisons tailored to Mansfield-area care. You will learn how osseointegration, peri-implant health, crown materials, bruxism, and clinician technique affect outcomes; we will also show sample cost element comparisons and when bone grafting or alternative prosthodontic approaches become necessary. Finally, the guide outlines candidacy criteria and local care options — including how free consultations and financing can help you evaluate the best path forward. Throughout, keywords like dental implants, dental crowns, implant longevity, crown lifespan, osseointegration, and dental financing in Mansfield are woven into practical recommendations for long-term oral health.
What Are Dental Implants and How Do They Affect Longevity?
A dental implant is a tooth replacement system that replaces the root and supports a prosthetic crown by integrating with the jawbone; this biological integration is the primary reason implants can last decades. Osseointegration, the direct structural and functional connection between living bone and the implant surface, stabilizes the fixture and transfers chewing forces safely into bone, reducing resorption and preserving adjacent teeth. Implant longevity separates the durable fixture (the implant post) from the prosthetic components (abutments and implant crowns) that may need replacement over time. Understanding each component’s material properties, surgical placement, and maintenance needs clarifies why implants often outlast standalone crowns but still require ongoing peri-implant care to prevent complications like peri-implantitis.
The following table compares core implant components and their attributes to highlight which parts determine long-term outcomes.
This component comparison shows where durability derives and what requires periodic attention, and that distinction leads directly into a closer look at each component and material choice.
Component
Characteristic
Longevity / Notes
Implant post (fixture)
Material: titanium or zirconia; function: osseointegration
Lifespan: lifetime potential with proper osseointegration and maintenance; highest durability of implant system
Abutment
Material: titanium, zirconia; function: connects fixture to crown
Lifespan: may require replacement if damaged or esthetic change needed; generally long-lasting
Implant crown (prosthesis)
Material: porcelain, zirconia, PFM; function: restores occlusion and aesthetics
Lifespan: 10–15+ years depending on material, wear, and parafunctional forces
What Components Make Up a Dental Implant?
A dental implant system comprises three primary parts: the implant post (fixture) embedded in bone, the abutment that links the post to the tooth restoration, and the implant crown that restores function and aesthetics. The implant post is commonly titanium or zirconia, with titanium offering long-term track records for osseointegration and zirconia serving as a metal-free alternative for select cases. Abutment selection balances strength and appearance; titanium abutments are highly durable, while zirconia abutments can provide improved esthetics in the anterior zone. The implant crown’s material—porcelain fused to metal (PFM), full ceramic, or monolithic zirconia—determines resistance to fracture, wear characteristics, and cosmetic outcome. Choosing the correct combination of fixture, abutment, and crown tailored to occlusion and esthetic demands reduces mechanical complications and improves the overall lifespan of the implant assembly.
This breakdown clarifies why material choices at each level matter and sets up the next section about the biological process that makes long-term implant success possible.
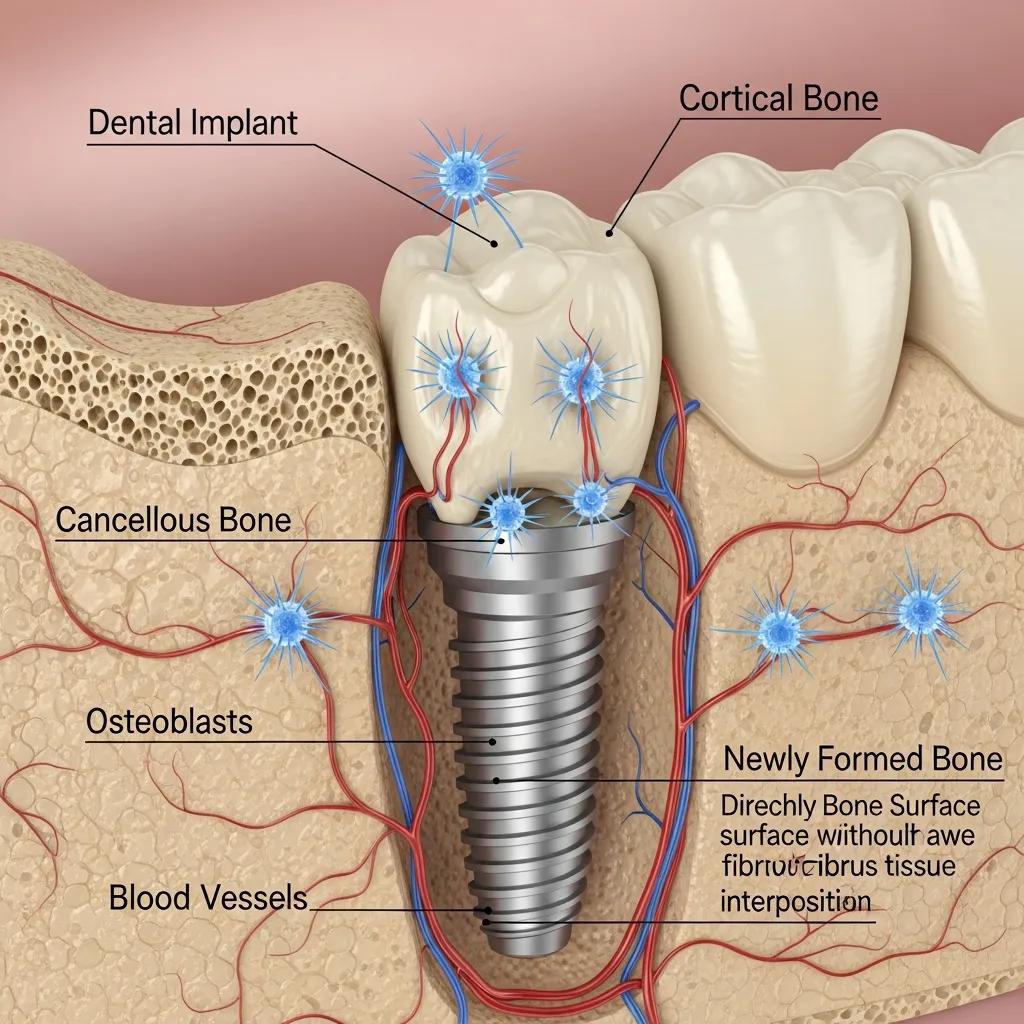
How Does Osseointegration Influence Implant Durability?
Osseointegration is the process by which living bone grows in intimate contact with the implant surface, creating a stable interface that allows the implant to function like a tooth root; successful osseointegration is the cornerstone of implant durability. The typical timeline for integration spans several weeks to months, with primary stability at placement followed by secondary biological stability as new bone forms; implant surfaces and surgical technique influence the speed and quality of this process. Risk factors such as smoking, uncontrolled diabetes, active periodontal disease, and poor bone quality increase the chance of integration failure or late peri-implant bone loss, while good oral hygiene, careful surgical planning, and atraumatic placement support success. Preventive measures—pre-op systemic health optimization, use of imaging for planning, and post-op hygiene protocols—reduce the risk of peri-implantitis, which is the leading biological cause of late implant failure. Understanding osseointegration’s timeline and risk profile helps patients plan realistic recovery expectations and emphasizes why maintenance and monitoring are essential for long-term durability.
Indeed, maintaining peri-implant health through strategic preventive measures and ongoing care is crucial for the sustained success of dental implants.
The long-term maintenance or restoration of peri-implant tissues‘ health depends on the strategic implementation of preventive measures and interventions. These measures should be initiated before implant placement and continued throughout a patient’s lifetime, as part of a tailored and comprehensive supportive peri-implant care (SPIC) programme. Central to the clinical efforts of maintaining and rehabilitating peri-implant tissues are several key factors, including the ongoing assessment and frequent monitoring of tissue health and stability, proactive oral health promotion, the control of risk factors and indicators and the provision of professional plaque biofilm removal. It is of paramount importance to underline that SPIC should not limit its scope exclusively to patients already in a state of peri-implant health; in fact, it is imperative that it should extend its protective effect to individuals who have been previously diagnosed and treated for peri-implant diseases, focusing on preventing its recurrence and progression, thereby avoiding further complications, such as implant loss.
Maintenance of peri-implant health in general dental practice, N Donos, 2024
Recognizing those biological risks naturally leads into the comparative lifespan discussion between implants and crowns to help patients weigh options.
What Are Dental Crowns and Their Typical Lifespan?
A dental crown is a prosthetic cap placed over a damaged or prepared tooth to restore shape, strength, and aesthetics, and its lifespan depends on material, tooth position, preparation quality, and maintenance. Crowns protect weakened tooth structure from fracture and can restore chewing function, but because they rely on the remaining tooth and its root health, they remain vulnerable to decay at margins and to periodontal issues that can undermine longevity. Typical lifespan ranges vary by material—metals and full-contour zirconia often last longer, while porcelain and PFM crowns sacrifice some durability for improved cosmetics—and clinical data frequently report average crown survival between 10 and 15 years with proper care. Material selection also depends on location in the mouth; posterior crowns need higher fracture resistance while anterior crowns prioritize translucency and esthetics. A concise comparison table below outlines common crown materials and expected durability to guide material selection based on function and cosmetic priorities.
Crown Material
Primary Attribute
Typical Lifespan
Porcelain (all-ceramic)
High esthetics, moderate strength
8–15 years depending on bonding and occlusion
PFM (Porcelain-Fused-to-Metal)
Balance of strength and esthetics
10–15+ years with good margins
Full zirconia
High strength, less translucent
10–15+ years for posterior restorations
Metal (gold, alloys)
Exceptional durability, limited esthetics
15–25+ years in functional zones
The table clarifies how material choice affects longevity and leads into the step-by-step process patients experience when receiving a crown.
What Types of Dental Crowns Are Available and How Do Materials Impact Durability?
Crowns come in several material classes, each with distinct failure modes and esthetic properties that affect longevity; choosing the right type depends on occlusal load, esthetic demands, and margin integrity. Porcelain and glass-ceramic crowns offer superior translucency for front teeth but have greater risk of chipping under high bite forces, while PFM crowns combine a metal substructure for strength with porcelain overlay for esthetics, balancing durability and appearance. Full-contour zirconia crowns deliver excellent fracture resistance for posterior teeth and bruxers but trade some translucency; metal crowns remain the most durable option where esthetics are not primary. Clinical recommendations often match material to tooth function: zirconia or metal for molars, PFM or all-ceramic for esthetic zones when careful occlusal design is employed. Understanding material-specific risks helps patients and clinicians select crowns that maximize lifespan without compromising function or smile appearance.
Choosing the appropriate material flows into the next topic: what patients should expect during the crown procedure and how that affects long-term outcomes.
What Is the Standard Procedure for Getting a Dental Crown?
The standard crown procedure follows predictable steps: tooth preparation, impression or digital scan, laboratory fabrication or same-day milling, and final cementation, with aftercare to maintain margins and occlusion. Most workflows include local anesthesia, removal of decayed or weak structure, shaping for adequate retention, and taking precise impressions or scans to ensure a well-fitting crown; temporary restorations protect the prepared tooth during fabrication. When same-day CAD/CAM systems are available, a single-visit crown can be milled and placed, while traditional lab fabrication typically requires two visits with a temporary crown in between; both approaches rely on accurate occlusal adjustments at placement. Aftercare includes avoidance of hard foods during initial settling, meticulous oral hygiene around margins, and periodic professional evaluations to detect early marginal breakdown or recurrent decay. Clear expectations about the procedural timeline and maintenance needs reduce the chance of early failure and prepare patients for the decisions that influence restoration longevity.
These procedural details naturally transition into a direct comparison of overall lifespan and performance between implants and crowns.
Which Lasts Longer: Dental Implants or Crowns?
Dental implants generally outlast dental crowns because the osseointegrated fixture resists decay and preserves bone, while crowns rely on remaining tooth structure that can fail from decay or fracture. In practice, the implant fixture (the titanium or zirconia post) can remain functional for decades, while the prosthetic crown or abutment may need periodic replacement; conversely, a crown placed on a natural tooth often needs replacement within a predictable timeframe due to margin issues or structural failure. When comparing average survival, implants demonstrate higher long-term survival for the fixture, whereas crown longevity is more variable and tied to the underlying tooth health and occlusal forces. For Mansfield patients weighing options, this means implants offer superior long-term tooth replacement in many clinical scenarios, but crowns remain appropriate when roots are healthy and saving natural tooth structure is a priority.
Quick comparative summary for snippet-style clarity:
Implant fixture lifespan: often several decades to lifetime potential; implant crown: 10–15+ years depending on material and care.
Natural tooth with crown lifespan: commonly 10–15 years, variable with decay risk and fit.
Maintenance: implants require peri-implant hygiene and monitoring; crowns require margin care and decay prevention.
This concise comparison leads into numeric lifespan details and the role of health and hygiene in real-world outcomes.
What Are the Average Lifespans of Implants Versus Crowns?
Numeric averages help set realistic expectations: implant fixtures commonly show survival rates exceeding 90–95% at 10 years in contemporary literature, while crowns typically average 10–15 years before requiring repair or replacement. Implant prosthetic components—crowns mounted on implants—tend to follow similar replacement timelines as natural-tooth crowns for veneering materials, so patients should expect periodic renewal of the visible crown even if the fixture remains stable. Variability is significant: patient factors such as bruxism, smoking, systemic disease, and local bone quality shift survival curves in either direction, and clinicians tailor materials and protective strategies accordingly. For practical planning, consider implants as an investment with higher initial cost but often lower lifetime replacement frequency for the foundational fixture, while crowns offer less invasive, lower-cost initial treatment but may require more frequent interventions over decades.
These lifespan figures naturally segue into how oral hygiene and systemic health modify individual outcomes.
How Do Oral Hygiene and Systemic Health Affect Longevity?
Oral hygiene and systemic conditions directly influence both implant and crown survival by altering infection risk, bone metabolism, and tissue healing; consistent home care markedly improves outcomes for either restoration. Poor plaque control promotes peri-implant mucositis and peri-implantitis around implants and recurrent caries at crown margins, both of which accelerate failure risk; conversely, effective brushing, interdental cleaning, and regular professional maintenance reduce complication rates. Systemic factors—uncontrolled diabetes, smoking, osteoporosis, and certain medications—modify bone healing capacity and immune response, increasing the chance of implant integration failure or crown-related periodontal breakdown. Management strategies include coordinating care with medical providers, implementing smoking cessation, optimizing glycemic control, and using protective devices like nightguards for bruxism to reduce mechanical overload. Recognizing how health and hygiene interact with restorative materials enables personalized risk reduction plans and improves long-term function.
What Factors Affect the Durability of Dental Implants?
Implant durability depends on biological factors (bone quality, peri-implant tissue health), mechanical factors (occlusal forces, prosthetic design), and clinical factors (surgical technique, prosthetic connection). Bone volume and density determine primary stability and the capacity for osseointegration; inadequate bone may require grafting to create a predictable foundation. Mechanical overload from bruxism or misaligned occlusion can cause screw loosening, prosthetic fracture, or marginal bone loss if not managed proactively. Surgical planning, including three-dimensional imaging and precise placement, reduces biomechanical stress and improves prosthetic emergence profile, while implant surface technology and material selection influence biological response. Comprehensive preoperative assessment and evidence-based surgical and restorative protocols minimize risk and maximize the long-term success of implant therapy.
These general determinants lead into a more detailed look at bone quality and bruxism as two of the most impactful clinical factors.
How Do Bone Quality and Bruxism Impact Implant Success?
Bone density and volume are essential for initial implant stability and for long-term load distribution; low-quality or insufficient bone increases the risk of micromovement and failed osseointegration, often necessitating bone grafting or staged approaches. When bone is compromised, grafting techniques—socket preservation, block grafts, or particulate augmentation—restore volume but extend treatment time and may increase cost, so candidacy assessment is critical. Bruxism and high occlusal forces create repetitive overload that can fatigue implant components, fracture prosthetic crowns, or cause progressive marginal bone loss; protective measures such as occlusal adjustment, splint therapy, and selecting high-strength prosthetic materials help mitigate these risks. Early identification of parafunctional habits and appropriate mechanical protection are essential parts of implant planning that directly influence long-term outcomes.
What Role Does Dentist Expertise and Implant Material Play?
Clinician experience and careful planning play a major role in implant outcomes because precise surgical technique, correct implant positioning, and appropriate restorative design reduce complications and mechanical stress. Practitioners who use advanced imaging for treatment planning, follow evidence-based protocols for asepsis and loading, and select implant systems with documented performance create conditions for durable results. Implant material—titanium versus zirconia—presents clinical trade-offs: titanium has a long evidence base for osseointegration, while zirconia offers esthetic and metal-free advantages for selected patients but with a shorter long-term dataset. Patients should ask prospective providers about surgical planning workflows, complication management strategies, and prosthetic options to ensure choices align with their functional and esthetic goals. Evaluating provider skill and material rationale is part of reducing uncertainty and improving the expected lifespan of implant restorations.
These provider and material considerations transition into crown-specific durability factors to complete the restorative comparison.
What Factors Influence the Lifespan of Dental Crowns?
Crown lifespan is governed by material properties, occlusal forces, tooth preparation quality, and the health of surrounding gum and bone tissues; all these elements interact to determine when a crown may fail or require replacement. Crown margins that are poorly fitted or subgingival can harbor bacteria and lead to recurrent decay or periodontal inflammation, shortening functional life. Material-specific vulnerabilities—such as porcelain chipping or metal wear—combine with patient behaviors like bruxism to accelerate mechanical failure. Clinician skill in margin preparation, occlusal adjustment, and adhesive technique is equally critical to optimize longevity. Understanding these interacting factors helps patients and clinicians select restorative strategies that maximize durable function for both anterior and posterior restorations.
How Do Material Choice and Bite Force Affect Crown Durability?
Material selection determines the primary failure modes for crowns: ceramic and porcelain crowns risk chipping under heavy occlusion, PFM crowns may exhibit porcelain veneer fracture while retaining metal support, and full-metal crowns resist fracture but lack esthetic appeal. In high bite-force scenarios or for patients with bruxism, clinicians often prefer high-strength zirconia or metal-based restorations to reduce fracture risk, while anterior restorations can use layered ceramics for improved translucency with careful occlusal management. Bite force management strategies include occlusal equilibration, nightguard therapy, and strategic material choice to protect restorations. Matching material strength to functional demands while maintaining acceptable aesthetics is the core decision that influences how long a crown will function before repair or replacement is needed.
These material and occlusal considerations naturally connect to the biological environment where margin health matters.
What Is the Impact of Gum Health and Dentist Skill on Crown Longevity?
Healthy gingival tissues and accurate crown margins prevent microleakage, recurrent decay, and periodontal inflammation, which are frequent causes of crown failure; clinician skill in margin placement and soft-tissue management is therefore essential. If the crown margin impinges on the biologic width or allows plaque accumulation, chronic inflammation can lead to bone loss around the tooth and eventual restoration compromise; excellent periodontal health supports longer crown survival. Skilled clinicians employ precise impression or scanning techniques, proper provisionalization, and margin verification to achieve a tight seal and maintain soft-tissue health. Routine periodontal maintenance, patient adherence to hygiene, and timely professional monitoring detect early issues before catastrophic failure occurs. Maintaining gum health and ensuring precise restorative fit are coequal priorities with material selection for extending crown life.
How Do Costs Compare Between Dental Implants and Crowns in Mansfield?
Cost comparison between implants and crowns requires separating initial procedure costs from long-term maintenance and replacement probabilities; implants typically incur higher upfront expenses driven by surgery and implant components, while crowns are less invasive and less costly initially but may require more frequent replacement. Key cost drivers for implants include surgical fees, implant fixtures, abutments, possible bone grafting, and prosthetic crowns; for crowns, cost drivers include tooth preparation, crown material, and laboratory fees. Long-term value analysis weighs the potential need for repeated crown replacement against the implant fixture’s longer expected service life and the cost of managing complications like peri-implantitis or root canal failures on crowned teeth. For Mansfield patients, understanding financing options and free consultation opportunities helps translate cost comparisons into actionable treatment plans tailored to individual budgets and clinical needs.
Below is a cost-element comparison table that clarifies components to consider when estimating total lifetime cost.
Cost Element
Description
Typical Impact on Total Cost
Implant surgery
Placement of fixture and surgical fees
Major upfront cost; may include grafting if needed
Implant prosthesis
Abutment + implant crown
Medium to high; crown replacement possible over time
Crown procedure
Tooth prep + crown fabrication
Lower upfront cost per tooth but may recur with replacements
Maintenance/repair
Nightguards, hygiene visits, repairs
Ongoing moderate costs; accumulates over decades
This EAV-style breakdown shows implants concentrate cost early while crowns may generate repeated costs, leading naturally into financing explanations and local offerings for Mansfield patients.
What Are the Initial and Long-Term Costs of Implants Versus Crowns?
Initial implant costs include surgical placement, implant fixtures, abutments, and the implant crown; bone grafting or sinus lift procedures add cost and time when indicated. By contrast, a crown on a natural tooth requires preparation, impression or digital scan, and crown fabrication—typically a lower initial outlay but with the expectation of periodic replacement or repair. Long-term costs factor in the implant fixture’s typical resistance to biological failure versus the likelihood of crown replacement due to wear, chipping, or recurrent decay; over multi-decade horizons, implants may offer cost-effectiveness despite higher initial expenses in many cases. Exact local pricing varies, so sample estimates and individualized treatment planning during consultation are necessary to determine out-of-pocket obligations and long-term financial impact.
Understanding these cost patterns informs how financing can bridge access to preferred treatments based on long-term value and clinical suitability.
What Financing Options Are Available for Mansfield Patients?
Mansfield patients often find that flexible financing and consultation offers make comprehensive restorative care more accessible without sacrificing quality or longevity. Many practices in the area emphasize affordable payment plans and third-party financing to spread the initial cost of implants, while crowns frequently have easier short-term financing options given their lower initial price point. For patients comparing implants and crowns, discussing financing during a free consultation can reveal tailored payment schedules, eligibility for low-interest plans, and whether in-house options exist to reduce immediate financial barriers.
Scheduling a free dental consultation or a free implants consultation is a practical next step for Mansfield residents seeking definitive pricing, individualized financing proposals, and a clear cost-versus-longevity analysis from experienced clinicians.
Who Is a Candidate for Dental Implants Versus Crowns?
Candidates for dental implants typically include individuals with one or more missing teeth, adequate jawbone volume or willingness to have grafting, and good overall health that supports healing; candidates for crowns are those with damaged but restorable tooth structure and a healthy root. The fundamental difference lies in whether the tooth root remains viable: implants replace absent roots, whereas crowns cap and protect existing roots. Systemic factors, jawbone health, smoking status, and active infection all influence candidacy and may necessitate preparatory treatments to qualify for implant therapy. A structured self-assessment followed by professional evaluation helps patients determine the right pathway for restoration based on function, esthetics, and long-term prognosis.
Missing tooth check: Do you have one or more missing teeth or non-restorable roots?
Tooth restorable check: Is the tooth structure sufficient to support a crown without severe fracture or infection?
Health and bone check: Do you have adequate jawbone volume and general health that supports surgery?
Lifestyle factors: Are you a non-smoker or willing to modify risk behaviors that affect healing?
This self-checkflow guides patients to the appropriate next step and leads directly to understanding jawbone considerations that often determine final treatment choices.
What Self-Assessment Questions Help Determine the Best Option?
A concise self-assessment helps prioritize whether to consider an implant or a crown before professional evaluation; these questions highlight tooth status, function, and systemic risks. Key items include whether the tooth is missing or has a healthy root, whether pain or infection is present, the patient’s willingness to undergo surgery if needed, and habits like smoking or heavy grinding that affect outcomes. If the tooth is missing or the root is non-restorable, implants become the primary long-term solution; if the root is sound and the tooth can be conservatively prepared, a crown may preserve natural structure. This initial filter clarifies likely pathways and supports a focused discussion during a free dental consultation to confirm candidacy and define next steps.
These self-assessment guidelines naturally lead into how jawbone health specifically impacts the feasibility and timeline of implant therapy.
How Does Jawbone Health Influence Treatment Choice?
Jawbone density and volume determine primary implant stability and whether grafting procedures are necessary, affecting both timeline and cost for implant therapy; clinicians use imaging to assess bone and plan accordingly. When bone volume is insufficient, bone grafting or sinus augmentation can reconstruct the site but add surgical stages and healing time, whereas crowns avoid this requirement because they rely on the existing tooth root. Imaging with CBCT or other three-dimensional scans provides accurate assessment of bone quality, nerve position, and sinus anatomy—information critical to safe implant placement. Patients with reduced bone may still receive implants after augmentation, but trade-offs include longer treatment duration and additional cost; knowing bone status early streamlines decision-making and expectations.
Having reviewed candidacy and bone considerations, local practice characteristics and conversion options for Mansfield patients are discussed next.
Why Choose Dentist In Mansfield for Your Dental Restoration Needs?
Dentist In Mansfield- Dentures and Dental Implants (also operating as Affordable Dentist Near Me – Mansfield) provides a comprehensive approach to dental restoration with services that include dental implants, dental crowns, dentures, general and cosmetic dentistry, and specialty care such as endodontics and periodontics.
The practice highlights patient-centered value propositions that support access to care: Free Dental Consultation and Free Implants Consultation help patients evaluate options without financial commitment; affordable payment plans and financing options reduce upfront barriers; and extended hours, 24-hour online scheduling, and a friendly, spa-like environment improve convenience and comfort for Mansfield-area patients.
Their one-stop-shop model and stated focus on patient experience support coordinated treatment planning across restoration, periodontal health, and prosthodontic follow-through to maximize the longevity of dental work. If you are weighing implants versus crowns, taking advantage of a free consult with the team can deliver a site-specific plan that balances clinical outcomes with long-term cost-effectiveness.
What Are the Benefits of Free Consultations and Flexible Financing?
A free consultation or a free implants consultation provides an initial oral exam, imaging review when indicated, and a tailored treatment estimate without financial obligation, making it easier to compare implant and crown options based on clinical realities rather than generic price lists. During a consult patients receive a clear explanation of candidacy, recommended materials, anticipated timelines (including grafting if needed), and a realistic long-term maintenance plan. Flexible financing and affordable payment plans help patients choose treatments aligned with their durability goals by spreading costs over time and making higher-investment options like implants more attainable.
Scheduling a free consult is a low-risk way to obtain personalized information tailored to your dental health and budget, and it helps translate long-term value comparisons into actionable next steps.
How Does Our Experienced Team Ensure Longevity of Your Dental Work?
An experienced clinical team optimizes longevity by combining thorough diagnostic planning, evidence-based surgical and restorative protocols, and ongoing maintenance programs that include hygiene coaching and protective measures for high-risk patients. Use of advanced imaging for implant planning, precision prosthetic design, and attention to occlusion and soft-tissue management reduce mechanical and biological failure risks; skilled clinicians also educate patients on hygiene, nightguard use for bruxism, and signs of peri-implant or crown margin problems.
Follow-up care and scheduled maintenance visits allow early detection and minimally invasive interventions, which preserve restorations and prevent major complications. This integrated, patient-centered approach aligns clinical decision-making with the long-term objective: restorations that maintain function and esthetics for as long as possible.