How Bone Quality Affects the Lifespan of Dental Implants Compared to Dentures: A Comprehensive Guide for Mansfield Patients
Bone quality refers to the density, volume, and biological health of the jaw’s alveolar bone, and it directly determines how well a dental implant anchors and integrates over time. Poor bone quality reduces initial mechanical stability and slows osseointegration, increasing the risk of implant failure, whereas healthy bone supports long-term implant lifespan and function. This guide explains jawbone anatomy and the Misch bone density classification, describes how implants interact with bone to preserve structure, and compares traditional dentures with implant-supported solutions so Mansfield patients can make informed decisions. We will also detail grafting options that expand candidacy for implants and cover systemic and lifestyle factors that affect implant longevity. Near the end, you’ll find information about scheduling a complimentary bone assessment and consultation with Dentist In Mansfield– Dentures and Dental Implants so you can evaluate your options with Dr. Elvis Le. Read on to learn how jawbone health shapes outcomes and which restorative pathways best match your needs.
What Is Jawbone Health and Why Does Bone Density Matter for Dental Implants?
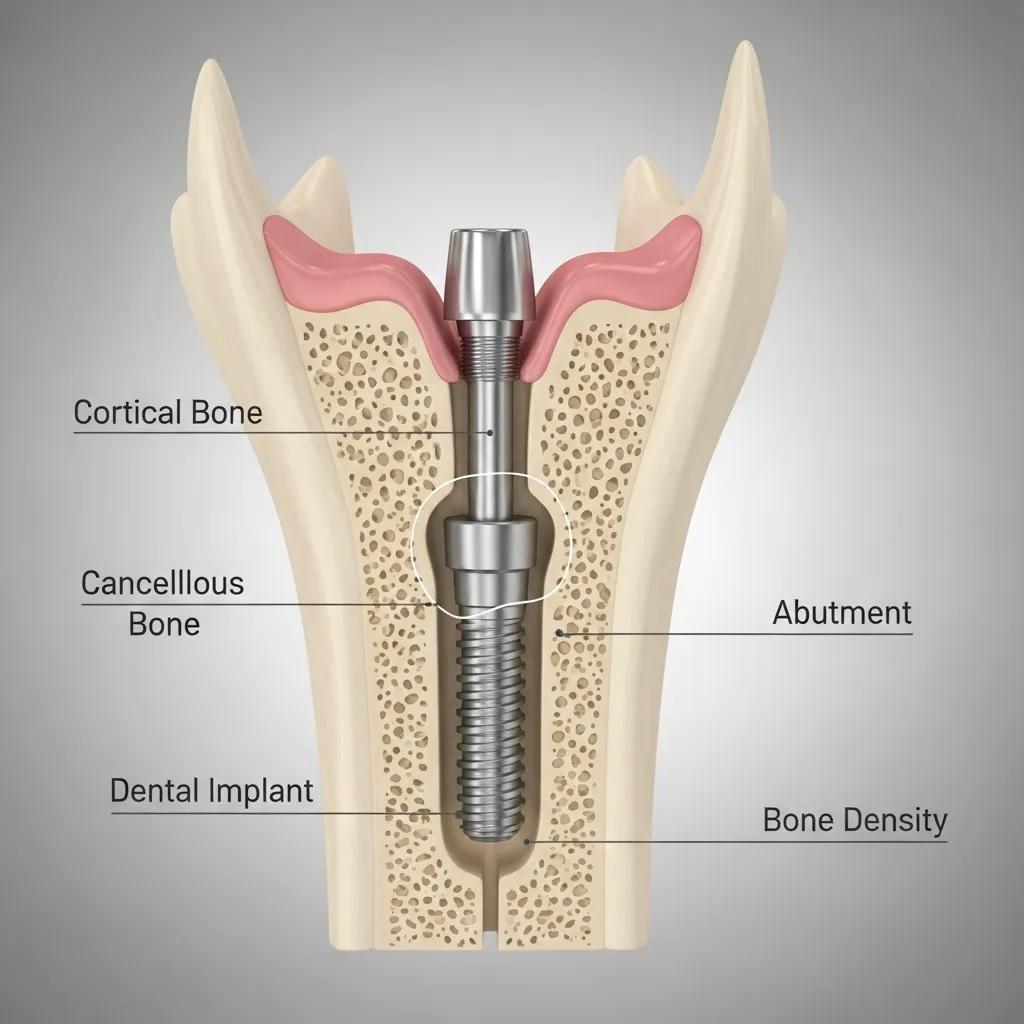
Jawbone health describes the structural integrity of the alveolar bone that supports teeth and dental restorations; bone density and volume determine mechanical support and biological potential for implant integration. Denser bone provides primary stability for endosteal dental implants and permits faster osseointegration, while low-density bone requires modified surgical techniques, slower loading, or adjunctive augmentation to reach comparable outcomes. Maintaining jawbone health preserves facial form and chewing function, and understanding bone quality helps clinicians select implant type, length, and timing for best long-term results. Clinicians use classifications such as Misch (D1–D4) and quantitative measures like Hounsfield Units from CBCT imaging to assess suitability; these metrics guide decisions about immediate loading, grafting, or selecting implant-supported dentures.
The following table summarizes common bone-density categories and their clinical implications to help patients visualize why density matters and how it affects treatment planning.
Bone Category (Misch)
Qualitative Density
Approx. Hounsfield Unit (HU) Range*
Clinical Implication
D1
Very dense cortical bone
> 1250 HU
Excellent primary stability; immediate loading often feasible
D2
Thick cortical + dense trabecular
850–1250 HU
Strong support; high success with standard protocols
D3
Thin cortical + porous trabecular
350–850 HU
Moderate stability; may need longer healing before loading
D4
Very porous trabecular
< 350 HU
Low initial stability; grafting or staged approach usually required
HU ranges are approximate benchmarks used by clinicians during CBCT/CT evaluation and vary by machine and protocol.
How Does Tooth Loss Impact Jawbone Density and Bone Resorption?
Tooth loss initiates a predictable biological response: the alveolar bone that once supported the tooth no longer receives functional loading and begins a resorptive remodeling process, often summarized as “use it or lose it.” Within the first six months after extraction, substantial vertical and horizontal bone loss can occur, reducing ridge height and width and compromising later implant placement. Patients commonly notice changes such as looser-fitting dentures, reduced chewing efficiency, and progressive narrowing of the dental arch; these clinical signs reflect the underlying bony volume loss. Smoking, periodontal disease, and delayed replacement accelerate resorption, while early implant placement or preservation techniques can minimize bone loss. Recognizing these timelines helps patients prioritize timely evaluation and consider grafting or implant options before bone loss becomes severe and more invasive reconstruction is required.
What Is the Misch Bone Density Classification and Its Role in Implant Success?
The Misch classification (D1–D4) stratifies jawbone into categories from very dense to very porous, giving clinicians a practical framework to anticipate implant behavior and tailor surgical protocols. D1 bone offers high insertion torque and immediate stability but can transmit greater stress to surrounding bone, while D4 bone provides little initial mechanical fixation and increases the likelihood of micro-movement during healing. This classification influences choices such as implant diameter and length, whether to use tapered designs for bicortical engagement, and the advisability of immediate versus delayed loading. In practice, cases with D3 or D4 bone often prompt preoperative planning for bone grafting, use of longer or wider fixtures, or staged approaches to maximize osseointegration. Understanding maneuverable options in each Misch category empowers patients to see why individualized imaging and planning are central to predictable implant longevity.
How Do Dental Implants Interact with Bone Quality to Affect Their Lifespan?
Dental implants rely on a biological process called osseointegration—direct structural and functional connection between living bone and the implant surface—to provide a lifelong foundation for prosthetic teeth; the pace and quality of osseointegration depend heavily on bone quality. In denser bone, implants achieve greater primary stability and faster load-bearing capability, whereas porous bone requires careful surgical technique, possible use of bone-condensing protocols, and longer healing intervals to reach the same long-term survival rates. Implants also provide mechanical stimulation that preserves bone through functional loading, which contrasts with the pressure and tissue-borne distribution seen with removable dentures. Precise preoperative imaging—typically CBCT scans—lets clinicians measure alveolar height, width, and estimated density to plan implant size and placement; for patients in Mansfield, a complimentary implant consultation can include CBCT review and a personalized treatment discussion to clarify candidacy and next steps.
Osseointegration begins with initial stability at placement and progresses through bone remodeling where the implant fixture becomes ankylosed to surrounding bone; this biological bond resists micro-motion and distributes occlusal forces. Higher bone mineral density supports faster mineralization along the implant surface and reduces early micromotion that can disrupt healing. Clinically, implants placed in D1–D2 bone show excellent early success and can often be restored sooner, while D3–D4 cases may show slightly higher early failure rates unless augmented, staged, or placed with designs optimized for low-density bone. Recent research indicates that with proper technique and post-operative care, long-term survival rates for implants in varied bone qualities converge, highlighting the importance of individualized planning and maintenance.
To make these clinical differences tangible, the table below compares implant outcomes and practical management strategies across a range of bone qualities, offering an at-a-glance view of expected osseointegration pace, survival likelihood, and typical interventions.
Bone Quality
Primary Stability
Osseointegration Pace
Expected 10-year Survival*
Typical Clinical Response
High (D1–D2)
High
Fast
> 95%
Immediate or early loading possible
Moderate (D3)
Moderate
Moderate
90–95%
May require longer healing; careful prosthetic loading
Low (D4)
Low
Slow
85–90%
Consider grafting, staged approach, or wider implants
Survival percentages are illustrative clinical estimates; individual outcomes depend on systemic health, surgical technique, and maintenance.
How Do Dental Implants Stimulate Bone and Prevent Bone Loss?
Implants transmit functional occlusal loads through the prosthetic crown and abutment down into the implant fixture and into surrounding alveolar bone, creating mechanical strains that stimulate bone remodeling in accordance with Wolff’s law. This load transfer encourages osteoblastic activity and selective bone deposition around the implant, which stabilizes the fixture and helps maintain ridge dimensions that otherwise would resorb after tooth loss. Over time, controlled mechanical loading through well-designed prosthetics preserves bone volume and cortical thickness and reduces future need for augmentation when compared to tissue-borne appliances. Clinical evidence shows that implant-supported restorations slow vertical and horizontal bone loss, particularly when occlusion is optimized and peri-implant tissues are healthy. Effective prosthetic design and regular maintenance ensure that the mechanical benefits of loading translate into sustained bone preservation and longer implant lifespan.
What Are the Minimum Bone Density and Volume Requirements for Successful Implants?
While exact thresholds vary by implant system and clinician preference, practical benchmarks guide candidacy: clinicians often seek at least 6–7 mm of ridge width and 10–12 mm of vertical height for standard endosteal implants, along with a bone quality that can provide sufficient insertion torque—typically corresponding to D2–D3 on the Misch scale. In very low-density bone (D4) or narrow ridges, alternatives include wider-diameter or shorter implants, osteotome bone-condensing techniques, or staged grafting to build height and width before implant placement. Quantitative HU values from CBCT give additional context during planning, but clinical judgment incorporates soft-tissue condition, proximity to vital structures, and prosthetic needs. If native bone falls short of these benchmarks, predictable augmentation strategies exist to create a robust environment for long-term implant success.
In What Ways Do Dentures Influence Jawbone Deterioration and Bone Loss?
Removable dentures rest on mucosal tissue and distribute occlusal forces across the ridge surface, but they do not transmit physiological loading into the alveolar bone the way an implant root does; this lack of functional stimulation is a primary reason dentures are associated with progressive bone resorption. Over years of use, pressure points, uneven load distribution, and continual mucosal compression accelerate cortical thinning and trabecular loss beneath the denture base. The result is reduced denture retention and stability, progressively poorer chewing efficiency, and changes in facial proportions that many patients describe as “sunken” or aged appearance. For some patients, dentures remain the appropriate choice due to medical or financial constraints, but understanding their long-term impact helps patients weigh the trade-offs and consider implant-supported alternatives when preserving bone and facial structure is a priority.
To clearly contrast the biologic outcomes between implants and conventional dentures, the list below summarizes the primary mechanisms through which dentures accelerate bone loss and then contrasts them to implant-mediated preservation.
Lack of Functional Loading: Dentures do not channel occlusal forces into the alveolar bone, eliminating a key stimulus for bone maintenance.
Mucosal Compression: Continuous pressure from denture bases compresses tissue and accelerates cortical resorption beneath the prosthesis.
Micro-Movement and Friction: Movement of ill-fitting dentures creates focal stress points that can erode underlying bone over time.
This comparison highlights that while dentures restore appearance and basic function, they do not prevent the progressive skeletal changes that implants are designed to mitigate. The next section examines specific mechanisms and clinical signs patients should watch for as denture-related resorption advances.
How Do Traditional Dentures Accelerate Bone Loss Compared to Implants?
Conventional dentures transfer chewing forces to soft tissues rather than to bone, creating a non-physiologic environment that fails to trigger osteogenic remodeling. Over time, repeated tissue-borne loading and friction cause chronic pressure on the ridge, leading to resorption patterns that reduce height and width of the alveolar crest. Patients frequently experience sore spots, unstable retention, and a need for relines or replacements as the ridge shrinks; these prosthetic adjustments do not stop the underlying skeletal loss. In contrast, osseointegrated implants behave like natural tooth roots by transmitting loads into bone, maintaining density and preserving ridge form. Recognizing these mechanistic differences helps patients understand why implant-supported solutions often produce more durable functional and esthetic outcomes than removable dentures.
What Are the Long-Term Effects of Denture Use on Facial Structure and Fit?
Long-term denture use without underlying bone preservation leads to predictable facial changes: loss of vertical dimension from ridge resorption, reduced support for the lips and cheeks, and an older-looking lower third of the face. As bone volume diminishes, denture bases must be repeatedly relined or remade to maintain fit, yet each reline only compensates for volume loss without halting it. The maintenance burden increases with time—more frequent adjustments, lowered chewing efficiency, and potential dietary restrictions—all of which affect quality of life. Patients considering dentures should weigh these long-term trade-offs against the benefits of implant-supported approaches when facial support and stable prosthetics are important goals.
What Are Bone Grafting Procedures and How Do They Support Dental Implants?
Bone grafting is a reconstructive technique that restores alveolar height and width by placing biologically compatible material where native bone is deficient, creating a stable foundation for future implants. Grafting can be performed as a ridge augmentation, block graft, particulate augmentation, or sinus lift depending on the defect’s size and location; the goal is to provide sufficient volume and density to allow predictable osseointegration of implants. Successful grafting combines appropriate graft material, rigid stabilization, healthy soft-tissue coverage, and adequate healing time; when these factors align, grafts offer high success rates and expand candidacy for implants in patients who otherwise would be limited to removable prosthetics. The table below compares common graft types so patients can understand options, healing expectations, and typical indications.
Graft Type
Source
Typical Healing Time
Success Considerations
Autograft
Patient’s own bone (intraoral or extraoral)
3–6 months
Gold standard for integration; donor morbidity risk
Allograft
Human donor bone (processed)
4–6 months
Avoids donor site surgery; good osteoconductive properties
Xenograft
Animal-derived (e.g., bovine)
6–9 months
Long-term volume stability; slower remodeling
Synthetic
Hydroxyapatite/bioceramics
4–9 months
No disease transmission; variable resorption rates
What Types of Bone Grafts Are Used for Dental Implant Preparation?
Clinicians choose graft types based on defect size, location (anterior vs posterior), and whether sinus augmentation is needed; common approaches include particulate onlay grafts for horizontal augmentation, block autografts for severe ridge deficiency, and lateral or transcrestal sinus lifts when the posterior maxilla lacks vertical height. Autografts are favored when rapid incorporation is required and donor bone is available, while allografts and xenografts offer excellent volume with less donor morbidity and are commonly used for particulate fills and ridge preservation. Synthetic substitutes and biologic growth factors can supplement or replace natural grafts in select cases to promote predictable bone formation. The choice balances factors such as healing time, invasiveness, patient preference, and long-term dimensional stability to ensure implants can be placed in an environment that supports durable osseointegration.
What Is the Recovery Process and Success Rate of Bone Grafting?
Recovery from grafting commonly involves a brief initial postoperative period of swelling and discomfort controlled with medication, followed by staged healing where soft tissue protection and occlusal rest are emphasized for several weeks. Typically, clinicians allow 3–9 months of healing before implant placement depending on graft type and site, with standardized follow-up to monitor integration through clinical exams and imaging. Success rates for modern grafting techniques are high when proper case selection, sterile technique, and flap management are observed, and complications—such as graft exposure or infection—are relatively uncommon with appropriate care. Clear postoperative instructions, smoking cessation, and systemic health optimization improve outcomes, and successful grafting frequently converts patients who would otherwise be limited to dentures into implant candidates with long-term functional and esthetic benefits.
How Do Implant-Supported Dentures Help Preserve Bone Compared to Traditional Dentures?
Implant-supported dentures anchor prostheses to osseointegrated fixtures, transferring occlusal loads into peri-implant bone rather than compressing soft tissues; this biomechanical pathway stimulates bone remodeling and helps retain ridge dimensions that would otherwise atrophy beneath conventional dentures. By converting a tissue-borne prosthesis into a bone-borne or hybrid solution, implant-supported dentures reduce the rate of resorption, improve chewing efficiency, and often decrease the frequency of relines and remakes. There are several designs—locators, bar-retained, or fixed full-arch solutions—that balance patient preferences for removability versus fixed restoration, and clinicians choose the approach based on bone availability, patient dexterity, and prosthetic goals. For many patients, implant-supported dentures represent a cost-effective middle ground that preserves bone better than removable dentures while avoiding the expense of full-arch fixed implant bridges.
Below is a concise list of benefits that helps patients see why implant-supported dentures are frequently recommended when bone preservation and prosthetic stability are priorities.
Improved Bone Maintenance: Implants provide mechanical stimulation to surrounding bone, slowing resorption.
Enhanced Stability and Comfort: Prostheses are more stable during chewing and speaking, reducing sore spots.
Reduced Maintenance: Fewer relines and better long-term fit compared to conventional dentures.
What Are the Benefits of Implant-Supported Dentures for Jawbone Health?
Implant-supported dentures provide direct load transfer to alveolar bone, stimulating osteogenesis and preserving ridge height and width relative to tissue-borne removable dentures. This preservation translates into improved prosthetic retention and reduced prosthetic maintenance over time, as stable bone supports consistent fit and occlusal relationships. Patients often experience better chewing efficiency and nutritional intake, which contributes indirectly to overall health and satisfaction. Additionally, implant-supported prostheses can improve facial support and esthetics by maintaining vertical dimension, helping avoid the “collapsed” lower facial appearance associated with long-term edentulism. For many patients, these functional and esthetic benefits justify the initial investment and surgical planning required to place implants.
When Are Implant-Supported Dentures Recommended Over Other Options?
Implant-supported dentures are typically recommended when patients have sufficient bone volume to support at least two to four implants per arch (or after limited grafting), desire improved stability over conventional dentures, and prefer a solution that reduces maintenance while preserving jawbone. They are especially valuable when fixed full-arch implants are not feasible due to cost or medical considerations but the patient still wants improved retention and bone preservation. Contraindications include uncontrolled systemic disease, heavy smoking without cessation plans, or situations where surgical risk outweighs benefit; in such cases, conventional prosthetics remain appropriate. A personalized assessment, including imaging and occlusal analysis, determines whether implant-supported dentures provide the optimal balance of function, cost, and bone-preserving potential.
What Factors Beyond Bone Quality Affect the Lifespan of Dental Implants?
Although bone quality is a cornerstone of implant success, systemic health, local disease, prosthetic design, and patient behaviors strongly influence long-term outcomes as well. Conditions such as uncontrolled diabetes or osteoporosis can modify bone remodeling and healing capacity, while peri-implantitis—a localized inflammatory disease around implants—can undermine osseointegration if plaque control and professional maintenance are neglected. Prosthetic factors including occlusal overload, poorly fitting restorations, or unfavorable emergence profiles increase mechanical stress and biological risk. Lifestyle factors such as smoking and bruxism also elevate failure risk, whereas good daily hygiene and regular professional follow-up promote durability. Understanding these interacting variables helps patients and clinicians craft preventive strategies to extend implant lifespan beyond what bone quality alone would predict.
Daily Oral Hygiene: Thorough cleaning around implants and prostheses every day prevents biofilm accumulation.
Regular Professional Care: Scheduled maintenance visits allow early detection of peri-implant inflammation and prosthetic wear.
Lifestyle Modifications: Smoking cessation and controlled systemic diseases reduce biological risk to implants.
How Do Conditions Like Osteoporosis and Peri-Implantitis Impact Implant Longevity?
Osteoporosis can reduce bone mass systemically and may affect alveolar bone density, potentially complicating implant placement and early stability; however, with medical coordination and careful surgical planning, many patients with controlled osteoporosis successfully receive implants. Peri-implantitis, which involves bacterial infection and progressive bone loss around implants, poses a direct threat to implant survival and underscores the importance of plaque control, smoking cessation, and prompt treatment of mucosal inflammation. Evidence indicates that timely intervention for peri-implant mucositis and rigorous maintenance protocols reduce progression to peri-implantitis; conversely, uncontrolled local inflammation significantly increases the risk of implant failure. Collaboration between the dental team and medical providers ensures systemic conditions are optimized before and after implant therapy to maximize longevity.
What Role Does Patient Oral Hygiene and Lifestyle Play in Implant Success?
Patient-led hygiene and behavior are critical determinants of implant outcomes: consistent plaque control prevents inflammatory conditions, while habits such as smoking and heavy bruxism impose biological and mechanical stresses that reduce survival rates. A recommended home-care routine includes cleaning around implant abutments and prostheses with interdental brushes or floss designed for implants, coupled with antiseptic rinses when indicated; clinicians typically schedule professional maintenance every three to six months depending on risk profile. Addressing parafunctional habits through occlusal adjustment, nightguards, or restorative modification reduces overload and mechanical complications. Patient adherence to these measures fosters a stable peri-implant environment and maximizes the decades-long potential lifespan of modern dental implants.
Why Choose Dentist In Mansfield for Your Dental Implant and Denture Needs?
Dentist In Mansfield- Dentures and Dental Implants offers a patient-centered approach focused on education, comfort, and predictable outcomes for implant and denture care in Mansfield. The practice provides free dental consultation options—including complimentary implant and denture consultations and a new-patient dental consultation valued at $79—so prospective patients can receive an informed assessment without upfront commitment. The clinic emphasizes education-based care delivered in a relaxing, spa-like environment with friendly staff, flexible financing options, and acceptance of most PPO insurance plans to make restorative options accessible. Dr. Elvis Le leads the team and emphasizes personalized treatment planning using modern imaging and diagnostic protocols to evaluate bone quality, candidacy, and prosthetic pathways. For patients seeking thorough evaluation of jawbone density and implant candidacy, a free consultation includes imaging review and a tailored plan to discuss grafting, implant-supported dentures, or conventional prosthetics.
How Does Dr. Elvis Le and the Mansfield Clinic Ensure Personalized Bone Health Assessments?
Dr. Elvis Le and the Mansfield team begin with a comprehensive clinical exam and review of dental history, followed by targeted imaging such as CBCT scans and periapical or panoramic X-rays when indicated to quantify alveolar height, width, and estimated density. These diagnostic steps allow precise planning of implant position, angulation, and selection of implant size, and they identify when bone grafting or sinus augmentation is advisable to achieve long-term stability. The practice emphasizes patient education—explaining Misch classification findings, imaging results, and practical implications in plain language—so patients clearly understand the rationale for recommended procedures. This diagnostic rigor pairs with a calm, supportive environment to ensure patients are comfortable and informed before consenting to restorative or surgical care.
How Can You Schedule a Free Consultation to Evaluate Your Bone Quality and Treatment Options?
Scheduling a complimentary consultation with Dentist In Mansfield- Dentures and Dental Implants is straightforward: prospective patients can call the clinic at (817) 567-2529 or visit the office in person at 708 Hunters Row Ct #102, Mansfield, TX 76063 to arrange an appointment; the free consult includes a focused discussion of concerns, an initial exam, and imaging review as appropriate. When booking, you can indicate interest in implant or denture evaluation to ensure the visit includes the correct diagnostic workflow; the clinic’s friendly staff will explain what to bring and what to expect during the consultation. Typical items to bring include a list of current medications, recent dental records if available, and insurance information to review coverage and financing options. This accessible, no-obligation consult helps patients understand candidacy, potential grafting needs, and practical next steps toward a durable, bone-preserving restorative plan.
Call to Book: Contact (817) 567-2529 to speak with staff and schedule the free consultation.
Prepare Documents: Bring any prior imaging or dental records and insurance details to the appointment.
Consult Process: Expect an exam, imaging review, and a clear, individualized treatment discussion with options and next steps.
Free Dental Consultation: New patients may qualify for a complimentary evaluation valued at $79, which helps clarify needs with no initial cost barrier.
Education-Focused Care: The practice emphasizes explaining findings and options so patients make informed decisions.
Comfort and Accessibility: A relaxing environment, flexible financing, and acceptance of most PPO plans aim to reduce barriers to care.
This final overview completes the guide and prepares Mansfield patients to take the next step toward restorations that consider both bone health and life-long function.